{kind=link}
In a remarkable display of community-driven innovation, the Vaccination Action Network (VAN) has revolutionised vaccine uptake across multiple African nations. Funded by the Rockefeller Foundation and managed by Amref Health Africa, VAN’s mission was to increaseCOVID-19 vaccine coverage through localised effort. The use of local partners bolstered local approaches to enhance vaccine demand through channels such as local media and approaches, community influencers among other strategies. Implemented from December 2022 to April 2024, this ambitious project spanned Kenya, Uganda, Tanzania, Malawi, and Zambia, resulting in significant public health advancements.
The selected geographical regions for the project scope had very low immunisation coverage but
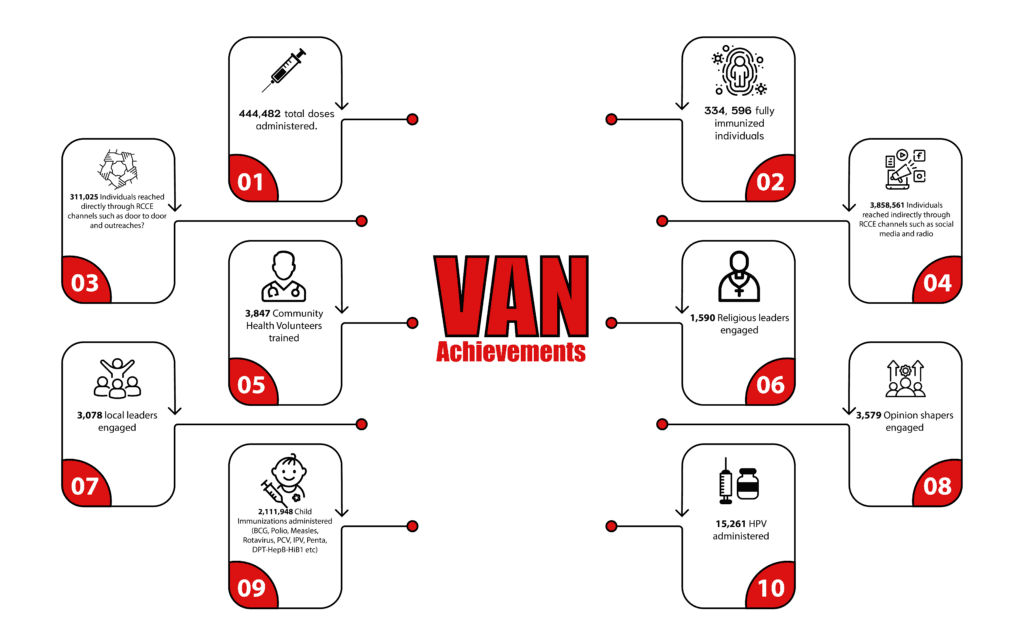
Many regions in Africa face daunting challenges in achieving high vaccination rates. Geographical isolation, cultural hesitancy, and logistical barriers often impede access to vaccines. VAN identified these obstacles and developed tailored approaches to address them, leveraging the strengths of local partners. As a result of this project’s efforts, some regions such as Zanzibar, Njombe among others have risen to at least over 70% immunisation coverage. Overall the project has administered 440,482 total doses with 334,596 individuals fully immunised.
Innovative Approaches and Success Stories
VAN Unique Approaches and Implementation Models
Vaccination Action Network is a multi-country project that was implemented from December 2022 to April 2024 in Kenya, Uganda, Tanzania, Malawi and Zambia. The project’s main goal was increasing vaccine uptake through local implementation hence the use of partners as below;
- Kenya; Population Services Kenya (PSK) and Panafricare
- Uganda; Infectious Diseases Institute (IDI) and Makerere School of Public Health (MAKSPH)
- Tanzania; Zanzibar Maisha Bora Foundation (ZMBF) and Community Concern for Orphans Development(COCODA)
- Malawi; Christian Health Association of Malawi (CHAM), Centre for Development Communication (CDC) and Self Help Africa (SHA)
- Zambia; Amref Health Africa Zambia (AHAZ) and Vision Outreach Zambia (VOZ)
A. COVID-19 Vaccination approaches
- Reaching the Unreachable in Kenya’s Flower and Sisal Farms.
In Nakuru, Kenya, flower farm workers often work long hours, making it difficult for them to access vaccination centers. The workers are picked up very early in the morning and often being dropped back late in the evening. The farms are often sealed off with minimal entry and at times a bit far from community settings. Population Services Kenya (PSK) tackled this by bringing vaccines directly to the farms. By setting up medical camps on-site, PSK ensured that these workers received their vaccinations without disrupting their demanding schedules. This initiative significantly boosted vaccination rates among a hard-to-reach population.
- Marketplaces in Zambia
In Chama, Zambia, bustling marketplaces provided a unique opportunity to reach a large audience. Vaccines were brought directly to these market hubs, making it convenient for people to get vaccinated while shopping. This approach not only increased vaccination rates but also integrated other health services, creating mini health centers in the heart of the community.
- Prisons and camps in Malawi
Prisons are often overlooked in public health initiatives. In Mulanje, Malawi, the Centre for Development Communication (CDC) targeted prisons and camps for displaced persons, ensuring these vulnerable populations received vaccinations. Following Cyclone Freddy, many were displaced, and setting up vaccination camps in these areas ensured widespread vaccine uptake among displaced persons and inmates.
- Leveraging Local Leaders in Kenya
In Turkana, Kenya, community trust was a significant barrier. The solution lay in leveraging the influence of local leaders. When the local chief publicly received the vaccine, it catalysed a wave of community acceptance, with many people following suit.
B. RCCE approaches
- Leveraging Local leaders in Kenya;
In Turkana, Kenya, largely inhabited by pastoralists with limited trust on vacinnes posed a great challenge to vaccine uptake in the community. The solution lay in leveraging the influence of local leaders. When the local chief publicly received the vaccine, it catalysed a wave of community acceptance, with many people following suit.In one community, after the chief was publicly vaccinated , the members flocked to the vaccination site in large numbers hence emphasising the influence of local leaders in promoting vaccine uptake.
- Religious leaders in Makueni, Kenya and Zanzibar;
Religious leaders in these regions played a pivotal role in promoting vaccination. In Makueni, a bishop’s public endorsement led to widespread vaccine acceptance. Similarly, in Zanzibar, a prominent Sheikh’s advocacy significantly increased vaccination rates in this predominantly religious and conservative community.
Zanzibar is predominantly a religious country hence very hesitant to introduction of health education. The Sheikh publicly got vaccinated and used his position in the mosque and the community to encourage more people to get vaccinated.
- Use of sports and Cultural Events in Malawi and Zambia;
Self Help Africa (SHA) used sports events to attract youth and disseminate vaccine information. Football tournaments, street theatre and local dances created engaging platforms to promote vaccine uptake. These events drew large crowds, providing a captive audience for health education and vaccination drives.
Effective data management was crucial to VAN’s success. Clearing data backlogs in Kenya and Tanzania ensured real-time updates and accuracy. Offline data monitoring and weekly situation room meetings in Zambia facilitated continuous assessment and strategic adjustments. Tools like community-led monitoring and demand creation interviews provided valuable insights, guiding targeted interventions and optimizing vaccine delivery.
C. Data Management and Routine Monitoring
- Clearing data backlogs in Kenya and Tanzania;
During vaccination, data clerks record clients’ details in hardcopy books or egistration forms. These paper-based records are intendedto simplify the later entry of data into the online government systems. Partners collaborated with local Ministry of Health (MOH) teams to address and clear any backlogs. The recorded data is carefully cross-referenced between the paper forms, the online MOH portal, and vaccine ledger books to ensure accuracy and consistency. Data entry is then conducted to resolve existing backlogs and align paper records with the vaccine ledgers. A notable example of this occurred in the Njombe, Makambako, and Ludewa councils in Tanzania, where COCODA supported the councils in clearing these backlogs. The backlog mainly resulted from the extensive door-to-door vaccination campaigns, which created challenges for real-time data updates due to limited staff and network connectivity issues.
In Kenya, particularly in Turkana and Makueni, the Panafricare team supported MOH teams in clearing backlogs, especially because mobile vaccination teams were deployed to remote areas with poor network connectivity, making it difficult to update client details on the ChanjoKe platform.
- Offline Data Monitoring;
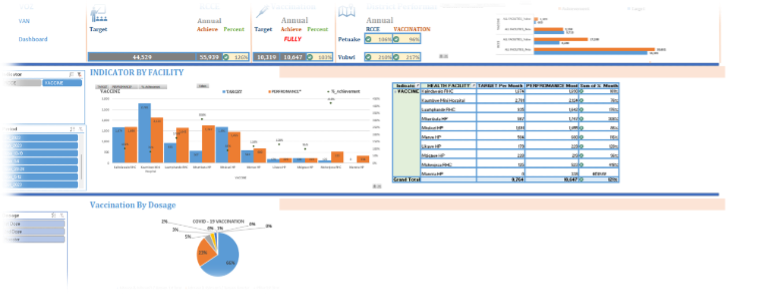
VOZ Team developed a parallel database for the project, independent ofthe government system to track performance. The offline database served as a backup for all the data stored in the government DHIS.
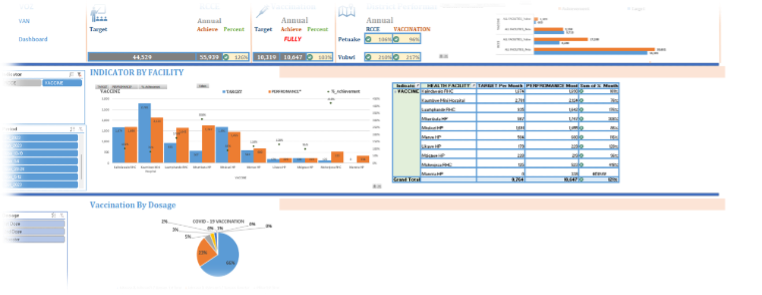
- Situation Room Meetings in Zambia;
VOZ team held weekly meetings with all their sites and District Health Offices to review key project and custom indicator performance. Insights from these meetings were used to inform programming.

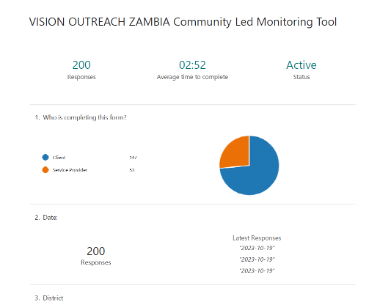
- Community-led Monitoring Tool in Zambia;
A community-led monitoring tool was used by VOZ to assess client satisfaction and service provisions after vaccination.


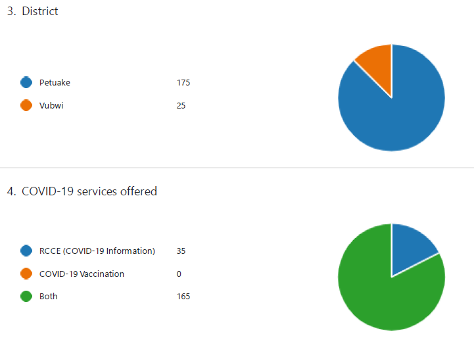
- Assessing source of information on COVID-19 vaccination for individuals accessing services at service points in Uganda;
The IDI team developed a tool to track which engagement methods among clients—whether healthcare workers, community healthcare workers, or community members—resulted in higher vaccine uptake. Before receiving the vaccine, clients were asked to indicate their primary source of information that prompted them to get vaccinated. The engagement channels included mobile demand creation vans, COVID-19 signage/banners, COVID-19 posters, vaccination champions, and healthcare workers at health facility service points.
According to healthcare workers, the most effective strategies for demand creation were community mobilisation drives using Public Address Systems on mobile vans, incorporating COVID-19 vaccination topics into other primary healthcare (PHC) discussions during health education talks at service points, and engaging vaccination champions during community drives. Community health workers identified mobile community mobilisation drives, health talks, and door-to-door mobilisation as the most effective strategies. Among all the channels, the mobile demand creation van emerged as the most preferred.
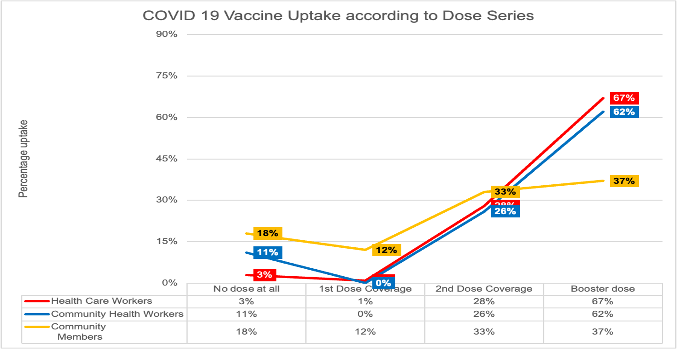
- Demand creation interviews to monitor project activities on the integration of COVID-19 vaccination into primary healthcare in Uganda;
The target group included healthcare workers, community healthcare workers, and community members. According to monitoring data routinely collected by IDI to guide implementation, individuals affiliated with the health profession are more likely to receive the COVID-19 vaccine. Healthcare workers and community health workers have the highest proportion of booster doses and the fewest unvaccinated individuals. In contrast, community members have the lowest proportion of booster doses and the highest number of unvaccinated individuals. This trend suggests that adherence to vaccination standards is highest among healthcare workers, followed by community health workers, with community members being the least adherent.
Caption/source[EA2] : The community lead monitoring tool by IDI
Pictorial board/Media files








Media links;
https://www.youtube.com/watch?v=5yDs1_f7_D4: Francis Matua ,ACK bishop talks about Covid 19 in Makueni.
https://www.youtube.com/watch?v=N20WBYrYpT8: A small remote village in Turkana leads in Covid19 vaccine uptake. Health worker explains why.
Author: Lily Achala, Monitoring and Evaluation Officer, GHS Unit